Endoscopic endonasal pituitary surgery, also known as transsphenoidal hypophysectomy, is a minimally invasive neurosurgical technique used to remove pituitary tumours and selected lesions at the skull base. The procedure is performed using an endoscope—a thin, rigid tube equipped with a high-definition camera and light source—which is inserted through the nostrils to reach the pituitary gland.
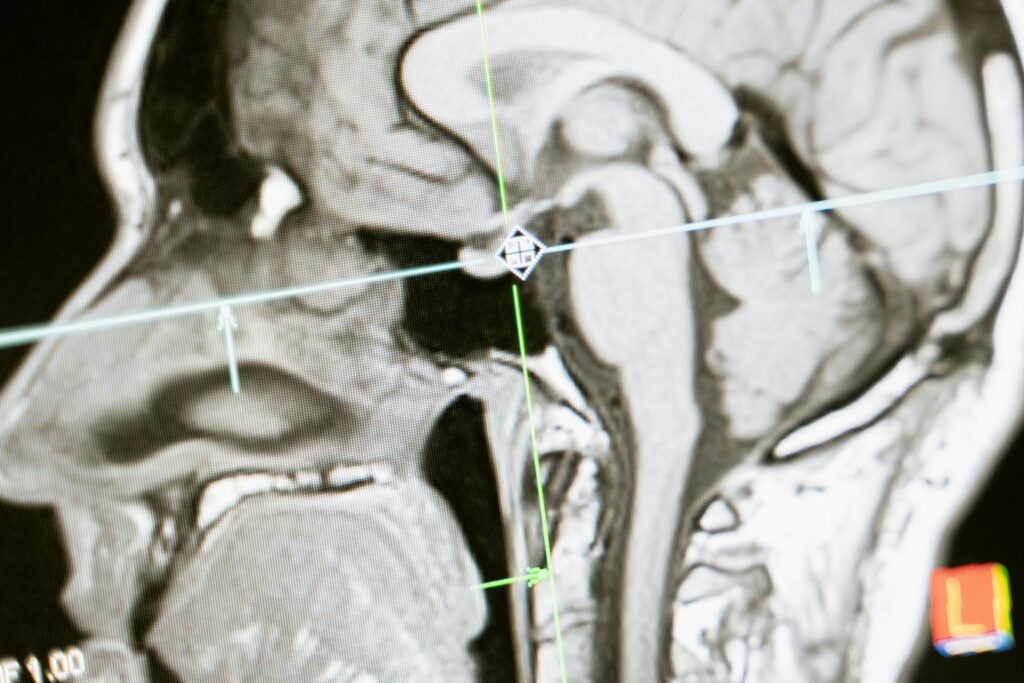
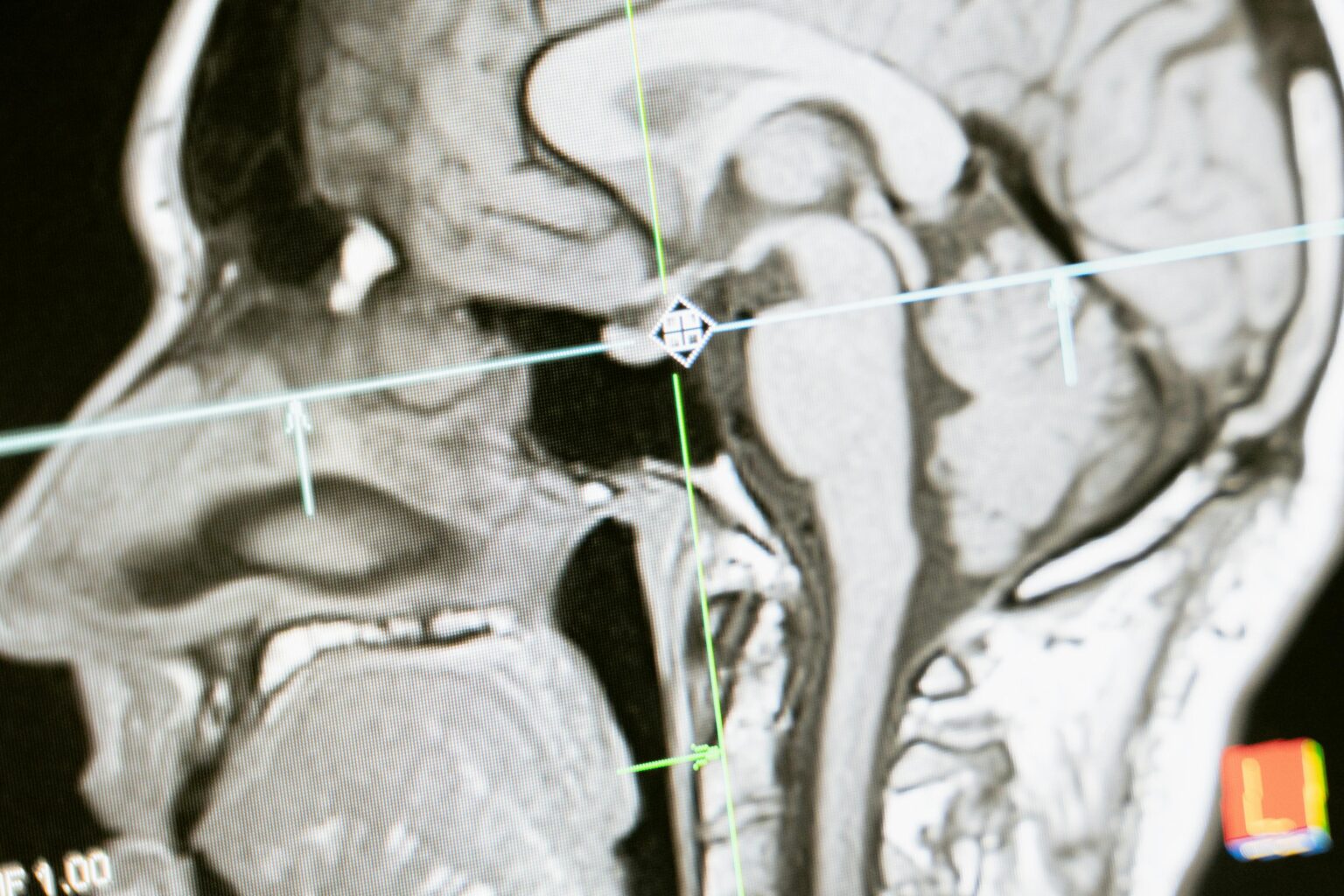
The pituitary gland is located within a small bony cavity known as the sella turcica, positioned behind the nose and between the eyes. Traditional surgical approaches to this region often required a craniotomy. In contrast, the endoscopic endonasal approach accesses the pituitary gland through the sphenoid sinus, a natural air-filled space located behind the nasal cavity.
Unlike traditional surgery, this approach provides a magnified, well-lit view of the surgical target, allowing the neurosurgeon to navigate with precision. It may be considered for the management of:
- Pituitary adenomas, including functioning and non-functioning tumours
- Craniopharyngiomas, which are rare tumours near the pituitary gland
- Rathke’s cleft cysts (fluid-filled sacs in the pituitary region)
- Brain cysts and Arachnoid cysts located in the sellar region
- Selected meningiomas (slow-growing tumours forming on the protective layers of the brain)
- Chordomas, which are rare bone tumours at the skull base
- Cerebrospinal fluid (CSF) leaks, where protective fluid escapes from the skull base